If you’ve spent any time around bodywork, physical therapy, or movement science in the last several years, you’ve probably heard the word “fascia.” It used to be the stuff anatomists ignored, the packing material they scraped away to get at the muscles and bones they actually wanted to study. That’s changed. Understanding fascia changes how you think about pain, posture, movement, and what it takes to create lasting change in your body.
I’m Tomer, a Certified Rolfer at Unify Rolfing in Toronto. Fascia is what I work with every day. Rolfing Structural Integration is a practice of working with the fascial system to reorganize the body’s structure. I want to share what I’ve learned from training and from thousands of hours of hands-on work about this tissue and why it matters for your health.
What is fascia?
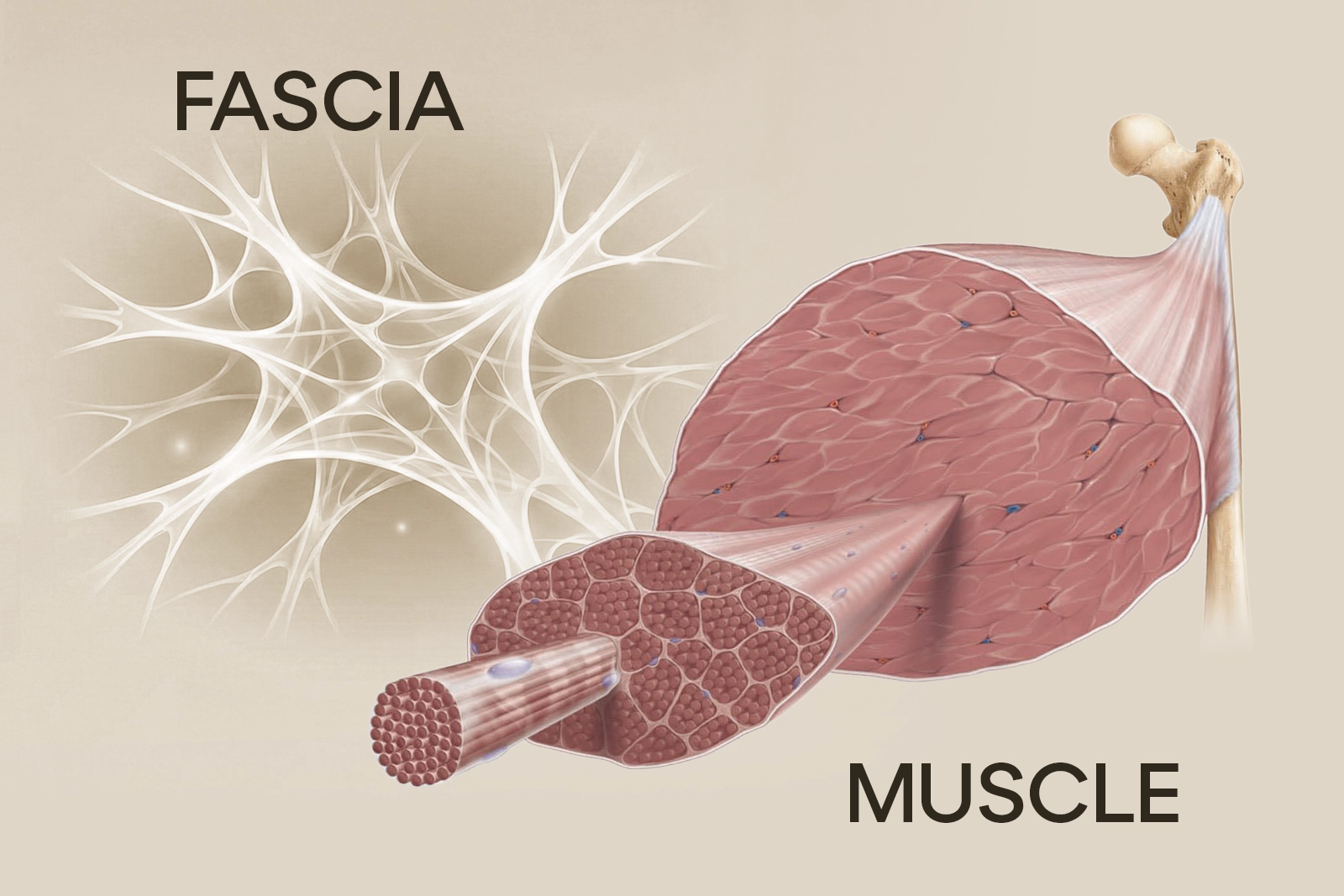
Fascia is a continuous web of connective tissue that runs through your entire body. It surrounds and penetrates every muscle, bone, nerve, blood vessel, and organ. If you’ve ever pulled the white membrane off a raw chicken breast, you’ve seen fascia. In the human body, it’s everywhere, and it does far more than that kitchen comparison suggests.
At the most basic level, fascia is made of collagen fibres (which provide tensile strength and structure), elastin fibres (which allow stretch and recoil), and ground substance, a gel-like matrix the fibres sit in. That ground substance can shift between a more fluid and a more solid state, which turns out to be central to how manual therapy works.
These components create a tissue that is strong and flexible at the same time. The exact composition varies by location and function. The thick, tough fascia of your IT band is very different from the delicate fascia surrounding your heart.
The layers
Fascia isn’t a single sheet. It exists in multiple layers throughout the body.
Superficial fascia sits just beneath the skin. It’s relatively loose, which lets the skin move over the structures underneath. It houses fat cells and provides insulation and cushioning.
Deep fascia is denser and more organized. It wraps around muscles, groups of muscles (forming compartments), bones, nerves, and blood vessels. This layer most directly influences your posture and movement patterns, and it’s the primary focus of Rolfing work.
Visceral fascia surrounds your internal organs, holding them in place while allowing the movement they need to function. Your lungs, heart, liver, and intestines are all suspended and supported by fascial structures.
Meningeal fascia surrounds the brain and spinal cord. The dura mater, the tough outermost layer protecting your central nervous system, is fascia.
These layers aren’t separate entities. They merge into each other, creating a continuous, interconnected system. Pull on one area and the tension transmits through the whole network.
Why everything is connected
This is what makes fascia interesting to me as a Rolfer: it doesn’t just wrap individual structures, it connects them. The fascia surrounding your calf muscle is continuous with the fascia of your hamstring, which is continuous with the fascia of your lower back, which is continuous with the fascia at the base of your skull.
This continuity is why a restriction in one area can cause symptoms somewhere entirely different. Your chronic headaches might trace to fascial tension in your feet. Your shoulder pain might originate from a fascial restriction in your opposite hip. These connections aren’t metaphorical. They’re anatomical.
Anatomist Thomas Myers mapped these connections into what he calls “Anatomy Trains,” longitudinal fascial lines running through the body. The Superficial Back Line, for instance, runs from the bottom of your feet, up the back of your legs, along your spine, over your skull, and down to your eyebrow ridge. Tension anywhere along this line affects the entire line.
This is one of the key reasons Rolfing takes a whole body approach rather than just treating where it hurts. If your lower back is bothering you, the source might live in your hamstrings, your calves, your deep hip flexors, or your ribcage. The body is a system. Treating it like a collection of independent parts misses the point.
I explain more about this approach on the Why Rolfing page.
How fascia becomes restricted
Healthy fascia is supple, elastic, and hydrated. It slides smoothly over adjacent structures and transmits force efficiently. But fascia is also highly responsive to how you use your body, and over time, several things cause it to become restricted, thickened, and stuck.
Injury and trauma
When tissue is damaged, whether from a sudden injury like a sprain or from surgery, the body lays down extra collagen as part of healing. This scar tissue is less organized and less elastic than healthy fascia. It works, but it creates areas of increased density and reduced mobility.
What matters here is that the body’s response to injury extends beyond the immediate site. When you sprain your ankle, the fascia throughout your leg, hip, and trunk adapts to protect the injured area. These compensatory patterns often persist long after the original injury has healed. You end up with restrictions that seem to have nothing to do with that old ankle sprain.
Chronic posture and repetitive movement
Fascia adapts to the demands placed on it. This is useful when those demands are varied and balanced. The tissue becomes stronger and more resilient in response to healthy stress. But when the demands are repetitive and one-directional, fascia responds by becoming denser and shorter in specific patterns.
Sitting at a desk eight hours a day, every day, for years, tells your fascia to shorten the front of your hips, round your upper back, and pull your head forward. The tissue literally remodels to accommodate the position you spend the most time in. This is why stretching alone often fails to fix postural issues. You’re trying to lengthen tissue that has structurally changed, not tissue that’s merely tight.
Runners develop fascial patterns specific to the sagittal plane (forward and back). Cyclists develop patterns shaped by the hunched, hip-flexed position. Swimmers develop patterns shaped by overhead rotation. Any repetitive movement, no matter how healthy the activity, creates asymmetric fascial adaptation over time.
Stress and emotional holding
Fascia is densely innervated with sensory nerve endings. It contains more sensory receptors than muscle tissue. This means it’s deeply connected to your nervous system and, by extension, to your emotional and psychological state.
Chronic stress causes the body to maintain a state of low-grade muscular tension: elevated shoulders, a clenched jaw, a braced belly. Over time, the fascia in these areas adapts to the constant tension, becoming denser and less pliable. The emotional pattern becomes a physical pattern, which becomes a structural pattern.
This is not a fringe concept. Research published in journals like the Journal of Bodywork and Movement Therapies has documented the relationship between fascial tone and autonomic nervous system activity. Your fascia is, in a real sense, a physical record of your stress history.
Dehydration and aging
The ground substance in fascia, that gel-like matrix, requires adequate hydration to maintain its fluid properties. Dehydration, whether from insufficient water intake or chronic inflammation, causes the ground substance to become more viscous and less mobile.
Aging also changes fascial properties. Collagen cross-linking increases with age, making the tissue stiffer and less elastic. This is natural, but it accelerates significantly with inactivity, dehydration, and chronic postural stress. The good news is that fascia remains responsive to intervention throughout life. It just requires more patient, sustained work as we age.
How restricted fascia causes pain and movement problems
When fascia becomes restricted, the effects ripple through the body in several ways.
Compression of nerves and blood vessels
Tight, thickened fascia can compress the nerves and blood vessels that pass through it. This causes pain, numbness, tingling, and reduced circulation. Many conditions that appear to be purely muscular or neurological, including some cases of sciatica, thoracic outlet syndrome, and carpal tunnel syndrome, have a significant fascial component.
Altered movement patterns
Restricted fascia limits range of motion and changes how forces are transmitted through the body. When one area can’t move freely, adjacent areas compensate by moving more than they should. Over time, these compensatory patterns create wear and tear in the overworked areas, leading to pain in structures that were never the original problem.
Reduced proprioception
Fascia is rich in proprioceptors, the sensory receptors that tell your brain where your body is in space. When fascia becomes restricted and adhered, the quality of proprioceptive information degrades. This leads to decreased coordination, balance problems, and a general sense of feeling disconnected from your body.
Chronic pain cycles
Restricted fascia creates self-reinforcing pain cycles. Restricted tissue causes pain, pain causes guarding and further tension, further tension causes more restriction, and more restriction causes more pain. Breaking this cycle requires addressing the fascial restrictions directly, not just the pain signals.
The science of fascial plasticity
The part of this story I find most encouraging: fascia changes. It responds to mechanical input. The tissue can and does reorganize in response to skilled manual work, movement, and sustained pressure.
The scientific basis for this is a property called thixotropy, the tendency of the fascial ground substance to become more fluid when mechanical energy (pressure, movement, heat) is applied. When I apply slow, sustained pressure to restricted fascia, the ground substance transitions from a more solid (gel) state to a more fluid (sol) state, allowing the collagen fibres within it to reorganize.
Research by Dr. Robert Schleip and others at the Fascia Research Congress (a biennial international conference running since 2007) has shown several things worth knowing:
- Fascia contains contractile cells called myofibroblasts that can actively stiffen or relax the tissue, independent of muscular contraction
- Sustained mechanical input changes the firing rate of fascial mechanoreceptors, which influences muscle tone through the nervous system
- Fascial tissue responds to manual therapy with measurable changes in density, hydration, and elasticity
- These changes can be both immediate (through neural reflexes) and longer-term (through tissue remodeling)
This dual mechanism, immediate neural change plus gradual structural remodeling, explains why you can feel different on the Rolfing table right away, and why the changes continue to develop for days and weeks afterward.
How Rolfing works with fascia
Rolfing Structural Integration was one of the first bodywork modalities to recognize fascia as the key to structural change. Dr. Ida Rolf developed her method in the mid-20th century, decades before fascia research became mainstream, because she observed that working with connective tissue produced more lasting structural change than working with muscles alone.
What makes Rolfing’s approach to fascia different from other bodywork:
Unlike massage, which typically uses faster, more rhythmic strokes directed at muscles, Rolfing applies slow, sustained pressure that engages the fascial layers specifically. The pace is deliberate. A single stroke might take 30 seconds or more, because fascial tissue requires sustained input to undergo thixotropic change.
A Rolfer is trained to differentiate between the multiple layers of fascia and to work with each layer on its own terms. The superficial fascia, deep fascia, and the fascia within muscles (perimysium and endomysium) all respond differently and require different approaches. This layered precision is specific to Rolfing training.
Rather than addressing the area where you feel pain, Rolfing follows a systematic strategy (often the Ten Series) that addresses fascial restrictions throughout the entire body. Restrictions in your foot can affect your hip. Restrictions in your ribcage can affect your neck. Lasting change requires reorganizing the whole fascial web, not just spot-treating.
I also frequently incorporate client movement during sessions. I might ask you to breathe, flex your foot, or turn your head while I’m working on a specific area. This engages the nervous system and helps the fascial changes integrate with your movement patterns in real time, rather than simply releasing tissue in isolation.
For more on how Rolfing sessions work in practice, visit the Sessions page.
Signs your fascia may need attention
You don’t need a medical diagnosis to recognize that your fascia might benefit from skilled work. These are the patterns I see most often in my practice:
Stiffness that doesn’t respond to stretching. If you’ve been stretching faithfully and your flexibility isn’t improving, or it improves temporarily and then snaps back to the same restricted range, the limitation is likely fascial, not muscular. Muscles respond relatively quickly to stretching. Fascial adhesions and structural shortening require different input.
Pain that moves around. If your pain shifts locations, lower back one week, hip the next, shoulder after that, this pattern often indicates fascial restrictions creating a cascade of compensations. The pain shows up wherever the compensatory chain is currently under the most stress.
A sensation of being “stuck” in your body. Many people describe this as feeling stiff, compressed, or like they’re wearing a suit that’s one size too small. This sense of restriction often reflects widespread fascial tightness, particularly in the superficial fascial layer.
Poor posture that takes effort to correct. If standing up straight requires constant muscular effort and quickly becomes tiring, the issue is likely fascial. When fascia is properly organized, good posture is effortless. It’s the resting state of a balanced structure, not something you have to muscle your way into.
Lingering effects from old injuries. That knee surgery from five years ago, the whiplash from the fender bender, the broken collarbone from childhood. If you still feel the effects even though the structures have technically healed, fascial adhesions and compensatory patterns are likely involved.
Chronic tension that returns despite treatment. If massage, heat, or muscle relaxants provide temporary relief but the tension always comes back, the underlying fascial pattern hasn’t been addressed. Muscles relax when the fascial container around them allows them to.
Reduced body awareness. If you feel disconnected from certain parts of your body, or if your coordination and balance have declined without a clear neurological cause, fascial restrictions may be degrading your proprioceptive input.
Taking care of your fascia
Beyond professional bodywork, several practices support fascial health.
Move in varied ways. Fascia thrives on diverse movement. If your life is dominated by one movement pattern (sitting, running, cycling), actively introduce variety. Walk on uneven terrain. Swim. Dance. Practice movements that take your body through unfamiliar ranges of motion.
Stay hydrated. Fascial ground substance is roughly 70% water. Chronic dehydration directly impairs fascial function. Drink water consistently throughout the day.
Don’t just stretch, move through ranges of motion. Static stretching has its place, but dynamic movement that takes your joints through their full available range does more for fascial health. Practices like yoga, tai chi, and natural movement training are particularly good for this.
Manage your stress. Because fascia is so responsive to nervous system activity, chronic stress directly impacts fascial health. Whatever stress management practices work for you, meditation, breathing exercises, time in nature, social connection, they’re also fascia care practices.
Get skilled manual work. Self-care is valuable, but it can’t replicate what skilled hands accomplish. Professional fascia-focused bodywork like Rolfing can address deep restrictions and systemic patterns that foam rolling and stretching can’t reach.
Your fascia is telling you something
The body is intelligent, and fascia is one of its primary communication systems. Pain, stiffness, limited movement, and postural imbalance aren’t random malfunctions. They’re messages from a fascial system that has adapted as well as it can to the demands placed on it and is now asking for help.
If what you’ve read here matches your experience, Rolfing may be worth looking into. It’s a modality built entirely around understanding and working with fascia, developed for exactly the kind of patterns described above.
I’m happy to discuss your specific situation and whether Rolfing could help. You can reach me at 647-581-7018 or through the contact page. My studio is at 272 Roncesvalles Ave in Toronto.
Fascia changes. Sometimes it just needs the right input.